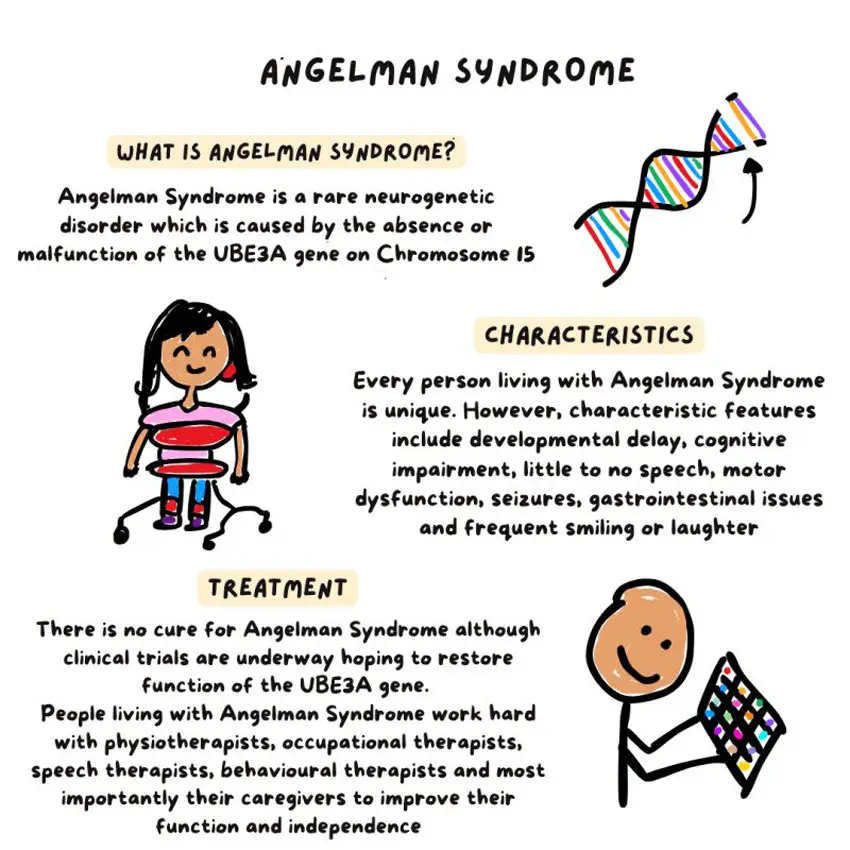
Angelman Syndrome is a rare neurogenetic disorder that affects neurological development, movement, communication, behaviour, and daily functioning. It occurs due to dysfunction of the UBEЗA gene located on Chromosome 15, which plays a crucial role in brain development and neural communication.
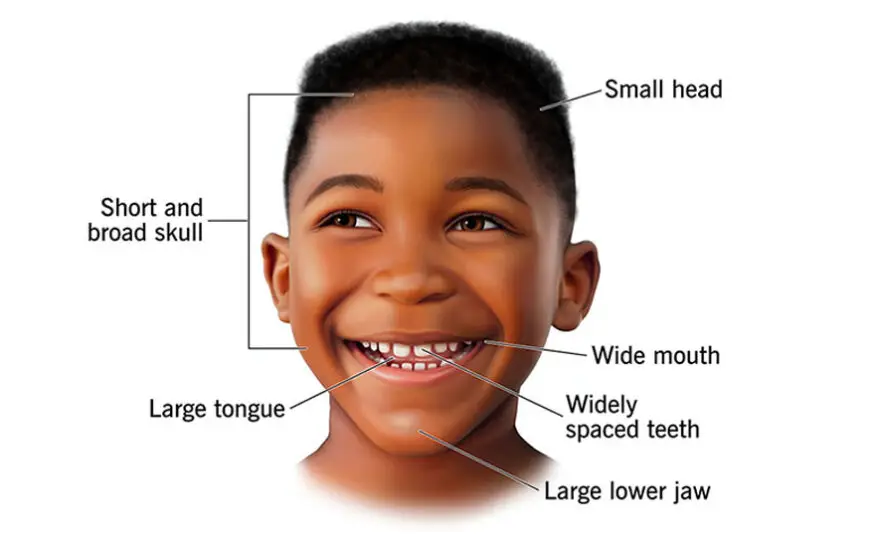
Children with Angelman Syndrome typically present with developmental delays, severe speech impairment, balance and coordination difficulties, seizures, sensory processing differences, and a characteristically happy and excitable demeanour. While there is no cure, early therapeutic intervention-especially occupational therapy-significantly improves functional independent participation in daily life.
This article focuses on the role of occupational therapy and therapeutic strategies that support development and quality of life. Understanding Functional Challenges.
Children with Angelman Syndrome often experience difficulties in: Sensory processing and regulation, Balance, coordination, and motor planning, Fine motor control and hand function, Feeding and oral-motor coordination, Attention and engagement, Self-care and daily living skills, Communication and social participation, Occupational therapy addresses these areas to enable meaningful participation in home, school, and community environments.
Importance of Early Intervention: Early therapy helps the developing brain build functional pathways and prevents secondary complications.
Intervention supports: Postural stability and motor control, Sensory modulation and attention, Independence in self-care, Functional communication, Participation in play and learning, A structured, individualized therapy plan produces the best outcomes.
Occupational Therapy: Core Areas of Intervention Occupational therapy (OT) aims to improve a child’s ability to perform daily activities independently and participate actively in life roles. Therapy is play-based, structured, and adapted to the child’s sensory and developmental needs.